
Research Article | DOI: https://doi.org/10.31579/2690-8794/044
1 Cell Biology and Neuroscience, Division of Life Sciences School of Arts and Sciences, Rutgers University, 604 Allison Road, Piscataway, NJ 08855.
*Corresponding Author: Garry F Merrill, Cell Biology and Neuroscience, Division of Life Sciences School of Arts and Sciences, Rutgers University, 604 Allison Road, Piscataway, NJ 08855
Citation: Ehmann PJ., Brush CJ, Bernard L., Dowden R., Ogilvie A., Wisniewski PJ, Piersol K., McCarthy T., and Merrill GF (2020) Influences on Blood Pressure in University Students, J.Clinical Medical Reviews and Reports. 3(1); DOI :10.31579/2690-8794/044
Copyright: © 2020, Garry F Merrill, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 September 2020 | Accepted: 20 October 2020 | Published: 03 February 2021
Keywords: young adults; blood pressure; time of day; male vs female
During Fall Semester, 2019, and Spring Semester, 2020, we had 287 students participate in a blood pressure measuring exercise. Subjects included both male (n=90) and female (n=197) students from multinational backgrounds and ethnicities. Pressures were measured traditionally and nontraditionally at 8:40 a.m., 1:40 p.m., and 6:40 p.m. Data were collected after the students had been instrumented and were lying quietly on a cot for 15-20 minutes (time for baseline data to reach steady state conditions). Both systolic and diastolic blood pressures were significantly greater in males than in females (P<0.05). Blood pressures were also significantly greater in the 6:40 p.m. group vs either 1:40 p.m. or 8:40 a.m. There was also a quadratic trend for blood pressures to be elevated in the morning group compared with the 1:40 p.m. group. Correlations between both systolic and diastolic blood pressures and BMI were also significant. BMI was a much stronger predictor of systolic (P<0.001) than of diastolic pressure (P<0.05). For every unit increase in BMI, systolic pressure increased 1.1 mmHg, and for each unit increase in BMI, diastolic pressure rose 0.4 mmHg. Results suggest that otherwise healthy young adult university students should be more aware of their blood pressure and the influences of obesity and overweight on it. They should try harder to achieve and maintain healthier lifestyles. This should include, but not be limited to, being more careful with their diets and being physically more active. Students should also avoid/limit unhealthy habits such as smoking, vaping, drinking (alcohol), and consuming caffeinated beverages.
Cardiovascular disease is still the leading cause of death and disability in industrialized nations, including the United States. Elevated blood pressure (hypertension) is a cardiovascular disease [1, 2]. In recent years the American College of Cardiology and the American Heart Association have redefined hypertension [1, 3-5]. Blood pressure categories in the new guidelines are: normal (normotensive): less than 120/80 mmHg; elevated: systolic pressure between 120-129 mmHg and diastolic pressure less than 80 mmHg; Stage 1hypertension: systolic pressure between 130-139 mmHg or diastolic pressure between 80-89 mmHg; Stage 2 hypertension: systolic pressure at least 140 mmHg or diastolic at least 90 mmHg; hypertensive crisis: systolic pressure over 180 mmHg and/or diastolic pressure over 120 mmHg [6]. Consistent with these definitions, patients need prompt changes in medications if there are no other indications of problems, or immediate hospitalization if there are signs of hypertension-mediated organ damage.
Few professionals and agencies seem to be concerned with the cardiovascular health of young adults, including college students. This lack of concern is unwarranted considering the numbers in this demographic population who choose to live unhealthy lifestyles such as poorly-timed consumption of foods and drinks (e.g. eating after midnight), over-eating, under-exercising, vaping, smoking, and excessive consumption of alcohol and caffeinated beverages such as coffee and energy drinks.
In Systems Physiology Laboratory (01:146:357, Rutgers University, New Brunswick, NJ, USA) we teach students experimental physiology, experimental design, and scientific writing (among other things). For example, we engage students in experiments that will help them learn about the cardiovascular system and how to care for it. We teach them about blood flow, blood pressure, and resistance to blood flow, heart rate and electrocardiography. Our course enrolls about twice as many female as male students (e.g. influence of ‘women in STEM’ emphasis at this institution). Many of them are planning to attend medical school or other health-related, post-baccalaureate graduate programs. Our course helps prepare them for medical and/or graduate physiology.
Subjects---Experimental subjects were students enrolled in Systems Physiology Laboratory at Rutgers University, New Brunswick/Piscataway, New Jersey. Students took our course either Fall, 2019, or Spring, 2020 (dates of data collection), and were all juniors or seniors from multicultural backgrounds (see Table 1) and a wide range of undergraduate majors (e.g. premed tracts, Biological Sciences, Kinesiology and Health, Marine Biology, Nutritional Sciences, etc.). They arrived at The Dr. Norman and Syril Reitman Systems Physiology Teaching Laboratory, Rutgers University, at either 8:40 a.m. or 1:40 p.m. or 6:40 p.m. Blood pressure data were collected about 45-60 minutes later when monitored cardiovascular variables were in the steady state.
Even though the course enrolls approximately 60 per cent young women, and 40 per cent young men, we made no further attempt to divide students according to ethnicities (e.g. Asian, Black, Caucasion, Hispanic, Indian, Latino, etc.). Nor were we able to collect data on lifestyles/habits that might have influenced outcomes. These are topics for follow-up investigation in this demographic group of experimental subjects.
Monitored cardiovascular variables included: heart rate (beats per minute, bpm), systolic blood pressure (BPsys), diastolic blood pressure (BPdia), mean arterial blood pressure (BPm), and finger plethysmography (microliters per cycle). A simple standard limb lead electrocardiogram (ECG, LLI) was also monitored. To help obtain these data a cardiomicrophone (model MLT201, AD Instruments, Colorado Springs, CO) was secured over the right brachial artery in the antecubital fossa using Tegaderm film (1624W, 3M Healthcare, St. Paul, MN). A pulse plethysmograph (model TN1012ST, AD Instruments, Colorado Springs) was attached to the index or middle finger. Signals from these physiological transducers were used to help identify systolic and diastolic blood pressures which were measured using a pressure cuff placed on the upper arm (model MLT0699 AD Instruments, Colorado Springs), and an electronic stethoscope (model ANR2, Think labs, Centennial, CO). All data were collected continuously using a data acquisition system (Power Lab, model 26T, 4-channel A-D converter running Lab Chart software, v. 8.1.16, December, 2019, AD Instruments, Colorado Springs) connected to a desktop computer (HP Compaq 8200 Elite, running Windows 10).
After students were instrumented they were instructed to lie as quietly and motionless as possible on a cot facing away from the computer and other equipment. When the above cardiovascular variables were in the steady state, the pressure cuff was inflated to about 200 mmHg for about 30 seconds before deflation. A second student research assistant placed the bell of the electronic stethoscope over the antecubital fossa and recorded both systolic and diastolic blood pressures. From these data a mean arterial blood pressure was calculated.
The experiment and statistical tests were designed a priori. Analysis of Variance (ANOVA) was used to detect initial variability among groups (e.g. male vs female and time of day). Tukey’s w-procedure was used to identify statistically significant differences among means. All data are expressed as means and one standard error of the mean (s.e.m.). Statistically significant differences were identified at the gold standard P<0.05 even though there were exceptions (e.g. P<0.001).
There were significant influences of gender, body mass, and time of day on both systemic mean arterial pressure and systolic and diastolic blood pressures (see Tables and Figures below). For example, regardless of time of day and body mass, blood pressures in males were significantly elevated relative to females. Also, pressures tended to be higher in the evening hours than in either the early afternoon or morning hours.
Relative to the more recent definitions of elevated blood pressure by the American College of Cardiology and the American Heart Association, the majority (66 per cent) of the 90 males in this study had some degree of hypertension. Hypertension was not as evident in the young women; in which case about 46 per cent of the 197 students showed evidence of hypertension. Still, of this group of 287 young adults, 150 or greater than fifty per cent showed signs of hypertension (Table 2, Figure 1).

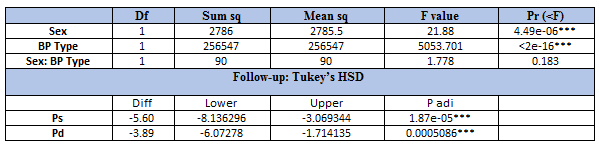

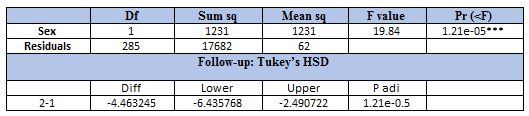
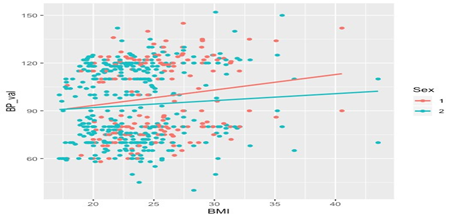
On the average systolic pressure was about 5-6 mmHg greater and diastolic pressure about 3.5 mmHg greater in males than in females (P<0.05). Also, the statistical correlation between gender and blood pressure was significantly greater for young men than for young women (Figs 1, 2). And, the correlation between systolic pressure and male gender was greater than that for diastolic pressure and male gender (see Table 3).

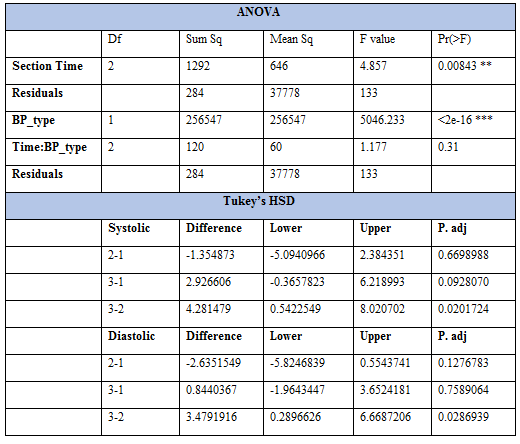
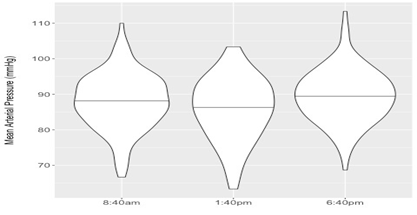
A distinct diurnal effect on blood pressure was also evident. This was statistically significant when comparing students in the 6:40 p.m. group with those in the 1:40 p.m. group (see Tables 4 and 5, Figs 3 and 4). As a rule, students in the evening sections had significantly higher blood pressures than those in the early afternoon sections (which also appeared to be reduced when compared with data in morning sections; although this comparison did not achieve statistical significance).


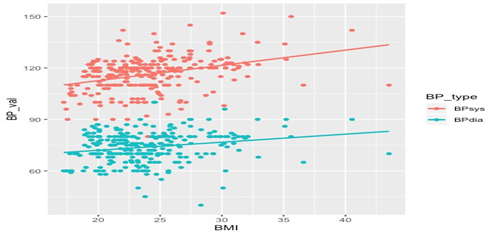
Blood pressure, whether mean arterial or systolic and diastolic, were also strongly dependent on body mass index in both genders (see Tables 6 and 7; also Figs 5-8). There was a positive statistical correlation between body mass index and blood pressure throughout the study (for both males and females). The statistical correlations revealed that young male students have higher blood pressure than young female students. The statistical slope relating blood pressure to body mass is significantly greater for males than females (Figs 5-8). Finally, the heavier the student, the higher the blood pressure. This was evident throughout the experiment, regardless of time of day or gender.



Gender and blood pressure---In the current experiment we found significant influences of gender, time of day, and body mass on both systemic mean arterial and systolic and diastolic blood pressures in university-age young adults. For example, regardless of time of day and body mass, blood pressures in males were significantly elevated relative to females. Similar observations have been made before [7-11] and mechanisms are still being worked out. For example, reductions in androgens are associated with reduced longevity, risk of fatal cardiovascular events, sarcopenia, osteoporosis, frailty, cognitive impairment, depression, sleep apnea, and atrial fibrillation [12]. As a result androgen supplements are commonplace today despite the fact that both males and females become hypertensive with their use [12].
The results for gender and blood pressure are summarized in Tables 1-3 and Figures 1 and 2. Despite the recent redefining of blood pressure by the American College of Cardiology and the American Heart Association, it is alarming that so many university students can be considered at or near hypertension (e.g. 66% of males in this study). We do not know the reasons for this. Clearly, however, most students live anxious (exams, papers), careless (late p.m./early a.m. hours; little and poor quality sleep) and even unfavorable lifestyles (poor diets, excess partying). Many student athletes do not fit the above characteristics, although participating in university sports is no guarantee of normotension or freedom from risk of cardiovascular disease [13, 14].
Timing and blood pressure---There was also a temporal (diurnal) component to the current results. Blood pressures tended to be higher in the evening hours than in either the early afternoon or morning hours. Statistical significance was only achieved, however, between the 6:40 and 1:40 p.m. sections. We also have no data to explain this observation, but educated speculation can do little harm. In the evening, data were collected between about 8-10 p.m. Thus, these students had already experienced a full-day’s activities, including eating evening meals between about 5-7 p.m. Having experienced a full-day’s activities was not the case when data were collected in either the 8:40 a.m. or 1:40 p.m. sections. It is not unreasonable to speculate that unhealthy hypercaloric evening meals, coupled with a subsequent, even if misguided, compensatory visit to the gym, and/or consumption of caffeine as a pre-workout ergogenic aid, individually and/or collectively contributed to the evening elevations in blood pressure. Of course more work is needed to support/reject such speculation.
Overweight and obesity and blood pressure---One of the most highly correlated variables with elevated blood pressure is body weight, usually expressed as body mass index (BMI) [15-21]. This was clearly the case in the current experiment. Whether male or female, enrolled in morning, afternoon or evening lab sections, overweight and/or obesity were significantly correlated with elevated diastolic, systolic and systemic mean arterial blood pressures.
Our students are sophisticated, bright juniors and seniors planning careers in medicine, the life sciences and research. They are aware of the connections between obesity, overweight, and blood pressure. Still, a fairly large fraction of them is overweight and hypertensive. This suggests that they lack the determination and discipline to achieve and sustain healthy lifestyles, including eating, exercising, and sleeping properly.
While COVID-19 paralyzed the world and created anxiety for everyone during the period February-April, 2020 (and beyond), overweight and obesity has been a worldwide pandemic (two plus generations) that currently afflicts 600 million adults and 40 million children under five years of age [20]. Its burden on international healthcare is mainly expressed by life-threatening co-morbidities including metabolic syndrome, type 2 diabetes and cardiovascular diseases including hypertension [21].
Related observations---In other students who took our course earlier we found a large group who responded atypically to a cold-pressor test [22]. In those students (exaggerated responders) both systolic and diastolic blood pressures rose 3-4 times more than they did in typical responders (about 72 per cent of the group exposed to the test). Related influences (gender, responses to stressors) have been reported by others in the four or five decades before our report [23-27]. Thus, there is additional evidence that overweight and obese young adults not only have elevated blood pressure, but might be at increased risk of other cardiovascular-related diseases as they age.
Finally, when it comes to healthy lifestyles and health-consciousness, university students, as a rule, are not the ‘gold standard’ the WHO, CDC, and like organizations should point to. Still, it goes without saying that such a declaration should exclude the hundreds and even thousands of dedicated, disciplined, student-athletes and others at colleges and universities who do Herculean jobs caring for their bodies and health. As two such examples consider the records of wrestlers Anthony Ashnault and Nick Suriano. Both are NCAA Division I, Big Ten Conference and National Champions, Rutgers University, 2019. We salute them and all like-minded university athletes!
In this course of nearly 350 students per year (175 in each of the two academic semesters), there are large populations who identify themselves as White, Black, Asian, Indian, Latino and Others. Regardless of race, gender, or time of day, there are many of these students who are borderline pre-hypertensive or hypertensive. Most are not even aware of their cardiovascular status until they participate in this experiment in Systems Physiology Laboratory. If asked, we advise them to see their physicians and to modify their lifestyles to include healthier diets and routine physical activity. We also instruct them in the irrefutable evidence linking obesity and excess body weight to hypertension. Still, more work and knowledge are needed on the cardiovascular health of college and university students.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
